Bài 30 – Tiếng Anh Y khoa: Viêm tuỵ cấp hoại tử do rượu * Acute necrotizing alcoholic pancreatitis
PCC fC Language – Thăng Long, Hà Nội, ngày 12/6/2026, Bài 30 của Chương trình Tiếng Anh Y Khoa do CLB Bóng đá PCC fC tổ chức đưa chúng ta đến với một ca bệnh nặng: viêm tụy cấp hoại tử do rượu, biến chứng sốc giảm thể tích, cổ trướng, tràn dịch màng phổi và tổn thương thận cấp thoáng qua. Đây không chỉ là một bài nghe IELTS Section 4. Đây là một bài luyện tư duy lâm sàng bằng tiếng Anh. Từ một cơn đau thượng vị sau uống rượu, người học phải lần theo mốc thời gian, nhận diện triệu chứng, hiểu dấu hiệu khám bụng, phân tích xét nghiệm, đọc ý nghĩa CT scan và lý giải vì sao bệnh nhân rơi vào sốc.
Với tinh thần “Khỏe – Vui – Hạnh phúc”, lớp học 5 giờ sáng không chỉ giúp chúng ta học thêm từ mới, mà còn giúp mỗi bác sĩ rèn luyện năng lực trình bày ca bệnh, giao tiếp quốc tế và từng bước trở thành người học, người dạy, người kết nối tri thức y khoa bằng tiếng Anh.
BÀI 30
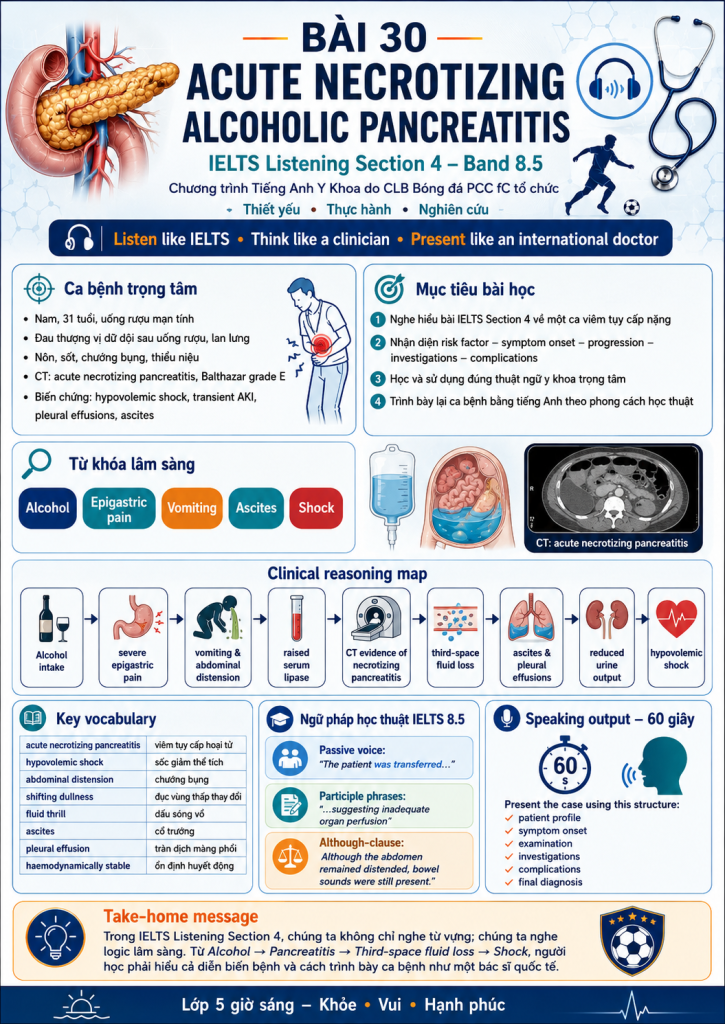
ACUTE NECROTIZING ALCOHOLIC PANCREATITIS
Severe pancreatitis – third-space fluid loss – hypovolemic shock
Chương trình: Tiếng Anh Y Khoa – Thiết yếu • Thực hành • Nghiên cứu
Đơn vị tổ chức: CLB Bóng đá PCC fC
Thời lượng: 05:00–05:25 sáng
Cấp độ: IELTS Listening 8.5
Đối tượng: Bác sĩ, học viên y khoa, người yêu tiếng Anh y khoa
Thông điệp: Listen like IELTS – Think like a clinician – Present like an international doctor.
Sĩ số: 48/98
1. Tên chủ đề bài học
From Epigastric Pain to Hypovolemic Shock: Listening to Severe Acute Pancreatitis as a Clinician
Tên tiếng Việt:
Từ đau thượng vị đến sốc giảm thể tích: Nghe – hiểu – trình bày một ca viêm tụy cấp nặng như bác sĩ quốc tế
2. Mục tiêu bài học
Sau bài học, học viên có thể:
- Nghe hiểu một bài IELTS Listening Section 4 về ca bệnh viêm tụy cấp hoại tử nặng.
- Nhận diện các thông tin then chốt: risk factor – symptom onset – progression – clinical signs – investigations – complications – final diagnosis.
- Sử dụng chính xác các thuật ngữ: necrotizing pancreatitis, third-space fluid loss, ascites, pleural effusion, hypovolemic shock, acute kidney injury.
- Trình bày lại ca bệnh bằng tiếng Anh theo cấu trúc học thuật.
- Phân tích các cấu trúc ngữ pháp cấp IELTS 8.5 trong văn phong y khoa.
3. Cấu trúc 25 phút buổi học
| Thời gian | Hoạt động | Nội dung |
| 05:00–05:03 | Warm-up | Nhận diện ca bệnh qua 5 từ khóa |
| 05:03–05:07 | Vocabulary activation | Từ vựng cốt lõi về viêm tụy cấp |
| 05:07–05:13 | Listening round 1 | Nghe lấy ý chính, bắt mốc thời gian |
| 05:13–05:18 | Listening round 2 | Điền từ IELTS Section 4 |
| 05:18–05:22 | Clinical reasoning | Vì sao bệnh nhân sốc? Vì sao thiểu niệu? |
| 05:22–05:25 | Speaking output | Trình bày ca bệnh trong 60 giây |
4. Warm-up: 5 từ khóa mở bài
Giáo viên chiếu 5 từ:
Alcohol – Epigastric pain – Vomiting – Ascites – Shock
Câu hỏi khởi động:
What disease do these five words suggest?
Gợi ý trả lời:
They suggest severe acute pancreatitis, most likely alcohol-related, complicated by third-space fluid loss and hypovolemic shock.
5. Transcript chuẩn cho bài nghe
Good morning everyone.
Today I would like to present a case of severe acute alcoholic pancreatitis complicated by hypovolemic shock.
The patient was a 31-year-old male mechanical worker with a history of chronic alcohol consumption of approximately 51.4 grams per day for eight years. He had previously been diagnosed with gastritis, but the condition had remained stable for several years.
The patient was apparently well until about twenty-one hours before admission, when he developed sudden severe abdominal pain shortly after drinking alcohol. The pain was initially located in the epigastric region but later radiated to the left upper abdomen and back.
Several episodes of vomiting followed. Initially, he vomited food contents, but later the vomitus became greenish-yellow. About three hours after symptom onset, fever developed and abdominal swelling gradually increased.
6. Key vocabulary – IELTS 8.5 Medical English
| Term | Pronunciation | Vietnamese meaning |
| acute necrotizing pancreatitis | /əˈkjuːt ˈnekrətaɪzɪŋ ˌpæŋkriəˈtaɪtɪs/ | viêm tụy cấp hoại tử |
| alcoholic pancreatitis | /ˌælkəˈhɒlɪk ˌpæŋkriəˈtaɪtɪs/ | viêm tụy do rượu |
| hypovolemic shock | /ˌhaɪpəvəˈliːmɪk ʃɒk/ | sốc giảm thể tích |
| chronic alcohol consumption | /ˈkrɒnɪk ˈælkəhɒl kənˈsʌmpʃən/ | uống rượu mạn tính |
| epigastric region | /ˌepɪˈɡæstrɪk ˈriːdʒən/ | vùng thượng vị |
| radiate to the back | /ˈreɪdieɪt tə ðə bæk/ | lan ra sau lưng |
| greenish-yellow vomitus | /ˈɡriːnɪʃ ˈjeləʊ ˈvɒmɪtəs/ | chất nôn xanh vàng |
| abdominal distension | /æbˈdɒmɪnəl dɪsˈtenʃən/ | chướng bụng |
| shifting dullness | /ˈʃɪftɪŋ ˈdʌlnəs/ | đục vùng thấp thay đổi |
| fluid thrill | /ˈfluːɪd θrɪl/ | dấu sóng vỗ |
| ascites | /əˈsaɪtiːz/ | cổ trướng |
| serum lipase | /ˈsɪərəm ˈlaɪpeɪz/ | lipase huyết thanh |
| third-space fluid loss | /θɜːd speɪs ˈfluːɪd lɒs/ | mất dịch khoang thứ ba |
| vasopressor therapy | /ˌveɪzəʊˈpresə ˈθerəpi/ | điều trị vận mạch |
| pleural effusion | /ˈplʊərəl ɪˈfjuːʒən/ | tràn dịch màng phổi |
| acute kidney injury | /əˈkjuːt ˈkɪdni ˈɪndʒəri/ | tổn thương thận cấp |
| haemodynamically stable | /ˌhiːməʊdaɪˈnæmɪkli ˈsteɪbəl/ | ổn định huyết động |
7. IELTS Listening Section 4 Practice
Questions 1–10
Complete the notes below.
Write NO MORE THAN THREE WORDS AND/OR A NUMBER for each answer.
Acute Necrotizing Alcoholic Pancreatitis
The patient was a 31-year-old male 1. __________ worker.
He had consumed approximately 2. __________ grams of alcohol per day for eight years.
The patient developed sudden severe abdominal pain about 3. __________ hours before admission.
The pain was initially located in the 4. __________ region.
It later radiated to the left upper abdomen and 5. __________.
The vomitus later became 6. __________.
At the district hospital, he received 7. __________.
On examination, the abdomen was markedly 8. __________.
Both shifting dullness and 9. __________ were positive.
CT scan demonstrated acute 10. __________ pancreatitis.
Answer key
- mechanical
- 51.4
- twenty-one / 21
- epigastric
- back
- greenish-yellow
- intravenous fluids
- distended
- fluid thrill
- necrotizing
8. IELTS 8.5 Challenge Questions
Questions 11–15
Choose the correct answer A, B, C or D.
11. What was the most likely underlying cause of the pancreatitis?
A. Gallstones
B. Alcohol use
C. Viral infection
D. Drug-induced injury
Answer: B. Alcohol use
12. Why was decreasing urine output clinically important?
A. It confirmed bowel obstruction
B. It suggested inadequate organ perfusion
C. It proved that the patient had liver failure
D. It indicated gastrointestinal bleeding
Answer: B. It suggested inadequate organ perfusion
13. What did positive shifting dullness and fluid thrill suggest?
A. Pleural effusion
B. Peritonitis only
C. Ascites
D. Intestinal obstruction
Answer: C. Ascites
14. Why was vasopressor therapy initiated?
A. The patient had persistent fever
B. The patient had unstable blood pressure
C. The patient had greenish-yellow vomiting
D. The patient had loose stool
Answer: B. The patient had unstable blood pressure
15. What did bilateral pleural effusions and persistent ascites reflect?
A. A localized gastric disorder
B. A widespread inflammatory response
C. Complete bowel obstruction
D. Chronic kidney failure
Answer: B. A widespread inflammatory response
9. Clinical reasoning map
From symptom to diagnosis
Alcohol intake
→ Sudden severe epigastric pain
→ Pain radiating to the back
→ Vomiting and fever
→ Raised serum lipase
→ CT evidence of necrotizing pancreatitis
→ Third-space fluid loss
→ Ascites and pleural effusions
→ Reduced urine output
→ Hypovolemic shock
10. Ngữ pháp học thuật trong bài
10.1. Passive voice trong trình bày ca bệnh
Các câu tiêu biểu:
- The patient was transferred to a tertiary referral centre.
- Additional investigations were subsequently performed.
- The disease was classified as Balthazar grade E.
- Vasopressor therapy was initiated.
- The patient was considered to have severe acute pancreatitis.
Công thức:
Subject + be + past participle
Ứng dụng trong y khoa:
- The patient was admitted to the ICU.
- Blood cultures were obtained.
- Mechanical ventilation was initiated.
- The diagnosis was confirmed by CT scan.
10.2. Participle phrases: cấu trúc “cho thấy rằng”
Các cụm rất hay:
- suggesting inadequate organ perfusion
- supporting the presence of ascites
- indicating that gastrointestinal transit was still preserved
- reflecting a widespread inflammatory response
Ví dụ nâng cấp IELTS 8.5:
Urine output progressively decreased, suggesting inadequate renal perfusion.
Thay vì nói đơn giản:
Urine output decreased. This suggested inadequate renal perfusion.
10.3. Although để mô tả đối lập lâm sàng
Câu trong bài:
Although the abdomen remained markedly distended, bowel sounds were still present.
Mẫu câu:
Although + abnormal finding, + preserved function.
Ví dụ:
- Although the patient remained conscious, his blood pressure was unstable.
- Although abdominal swelling persisted, gastrointestinal transit was preserved.
- Although renal function was initially impaired, urine output later improved.
11. Speaking practice – 60-second case presentation
At a district hospital, the patient received intravenous fluids. However, despite treatment, his abdominal pain and abdominal distension continued to worsen. At the same time, urine output progressively decreased, suggesting inadequate organ perfusion.
Because of the deteriorating clinical condition, he was transferred to a tertiary referral centre.
On arrival, he remained conscious but complained of dizziness, severe abdominal pain and mild shortness of breath. Physical examination revealed a markedly distended abdomen with evidence of free fluid within the abdominal cavity.
Both shifting dullness and fluid thrill were positive, supporting the presence of ascites.
Although the abdomen remained markedly distended, bowel sounds were still present. The patient continued to pass gas and reported loose yellow stool, indicating that gastrointestinal transit was still preserved.
Additional investigations were subsequently performed.
Laboratory testing showed a serum lipase level more than three times the upper limit of normal.
A contrast-enhanced CT scan demonstrated acute necrotizing pancreatitis. The disease was classified as Balthazar grade E, indicating extensive pancreatic and peripancreatic inflammation with significant fluid collections.
The CT findings corresponded to a high CT Severity Index score.
On the second hospital day, despite initial improvement, the patient developed recurrent hypotension due to ongoing third-space fluid losses and systemic inflammation.
Because blood pressure remained unstable, vasopressor therapy was initiated.
At that stage, the patient was considered to have severe acute pancreatitis complicated by hypovolemic shock.
Further assessment also demonstrated bilateral pleural effusions and persistent ascites. These findings reflected a widespread inflammatory response involving multiple serosal cavities.
Fortunately, following continued treatment, renal perfusion gradually improved. Urine output increased to approximately two thousand millilitres per day.
The patient remained conscious and cooperative. Although abdominal swelling and mild shortness of breath persisted, he was haemodynamically stable.
The final diagnosis was severe acute necrotizing pancreatitis secondary to alcohol use, complicated by hypovolemic shock, transient acute kidney injury, bilateral pleural effusions and ascites.
This is a case of severe acute necrotizing alcoholic pancreatitis complicated by hypovolemic shock.
The patient was a 31-year-old male mechanical worker with a long history of alcohol consumption. He developed sudden severe epigastric pain shortly after drinking alcohol. The pain later radiated to the left upper abdomen and back and was followed by repeated vomiting, fever, progressive abdominal distension and reduced urine output.
On arrival at a tertiary referral centre, he remained conscious but complained of dizziness, severe abdominal pain and mild shortness of breath. Physical examination revealed marked abdominal distension, positive shifting dullness and positive fluid thrill, suggesting ascites.
Laboratory testing showed serum lipase more than three times the upper limit of normal. Contrast-enhanced CT demonstrated acute necrotizing pancreatitis, classified as Balthazar grade E.
On the second hospital day, the patient developed recurrent hypotension due to ongoing third-space fluid losses and systemic inflammation. Vasopressor therapy was initiated. Further assessment showed bilateral pleural effusions and persistent ascites.
Following continued treatment, renal perfusion improved and urine output increased. The patient remained conscious, cooperative and haemodynamically stable.
12. Mini-drill: nói nhanh theo cụm
Giáo viên đọc tiếng Việt, học viên phản xạ tiếng Anh:
| Tiếng Việt | Tiếng Anh |
| đau bụng dữ dội đột ngột | sudden severe abdominal pain |
| đau lan ra sau lưng | pain radiating to the back |
| chướng bụng tăng dần | progressive abdominal distension |
| lượng nước tiểu giảm dần | progressively decreased urine output |
| tưới máu cơ quan không đủ | inadequate organ perfusion |
| dấu sóng vỗ dương tính | positive fluid thrill |
| cổ trướng dai dẳng | persistent ascites |
| mất dịch khoang thứ ba | third-space fluid loss |
| huyết áp không ổn định | unstable blood pressure |
| ổn định huyết động | haemodynamically stable |
13. Bài tập phát âm trọng điểm
Tập trung vào 5 từ khó:
- pancreatitis
/ˌpæŋkriəˈtaɪtɪs/ - necrotizing
/ˈnekrətaɪzɪŋ/ - hypovolemic
/ˌhaɪpəvəˈliːmɪk/ - ascites
/əˈsaɪtiːz/ - haemodynamically
/ˌhiːməʊdaɪˈnæmɪkli/
Câu luyện phát âm:
The patient was diagnosed with acute necrotizing pancreatitis complicated by hypovolemic shock, ascites and bilateral pleural effusions.
14. Clinical discussion bằng tiếng Anh
Question 1
Why can severe acute pancreatitis cause hypovolemic shock?
Suggested answer:
Severe acute pancreatitis can cause hypovolemic shock because systemic inflammation increases vascular permeability, leading to third-space fluid loss into the peritoneal and pleural cavities. As intravascular volume decreases, blood pressure falls and organ perfusion becomes inadequate.
Question 2
Why was urine output an important marker in this case?
Suggested answer:
Urine output was important because it reflected renal perfusion. The progressive decrease in urine output suggested inadequate circulating volume and possible transient acute kidney injury.
Question 3
Why did the patient still pass gas despite abdominal distension?
Suggested answer:
Although the abdomen was markedly distended, bowel sounds were still present and the patient continued to pass gas, indicating that gastrointestinal transit was preserved and complete bowel obstruction was unlikely.
15. Take-home message
In IELTS Listening Section 4, we do not only listen for words; we listen for logic.
Trong bài này, logic lâm sàng là:
Alcohol → acute pancreatitis → necrosis → inflammation → third-space fluid loss → ascites and pleural effusions → reduced organ perfusion → hypovolemic shock.
Người học giỏi không chỉ nghe được từ pancreatitis, mà còn nghe được diễn biến bệnh, mối quan hệ nhân quả, và cách bác sĩ trình bày một ca bệnh nghiêm trọng bằng tiếng Anh học thuật.
16. Khẩu hiệu poster cho Bài 30
BÀI 30 – ACUTE NECROTIZING ALCOHOLIC PANCREATITIS
Listen like IELTS.
Think like a clinician.
Present like an international doctor.
Từ đau thượng vị đến sốc giảm thể tích – học tiếng Anh bằng tư duy cấp cứu, hồi sức và độc chất.
PCC fC Language
Bài đọc thêm: